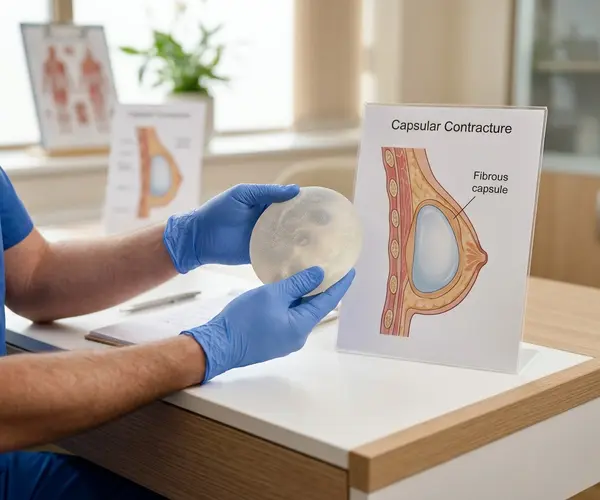
How Capsular Contracture Develops
After breast augmentation, the body responds to the implant by forming a thin layer of fibrous scar tissue around it. This is a normal biological reaction to any foreign material and is not inherently a problem. In most patients, this capsule remains thin, soft, and pliable, and the breast looks and feels natural.
Capsular contracture occurs when this process becomes excessive. The collagen fibres in the capsule begin to contract and thicken, gradually squeezing the implant. In mild cases, the breast may feel slightly firmer than expected. In more advanced cases, the breast can become visibly distorted, feel hard to the touch, and cause significant discomfort.
The exact mechanisms that trigger excessive capsule formation are not fully understood, but research has identified several contributing factors. Subclinical bacterial biofilm on the implant surface, haematoma (blood collection) around the implant, seroma (fluid collection), and individual variation in wound healing response all appear to play a role.
The Baker Grading Scale
Surgeons classify capsular contracture using the Baker scale, which has four grades.
| Grade | Description |
|---|---|
| I | The breast looks and feels natural. The capsule is soft and pliable. This is the normal, expected outcome. |
| II | The breast looks normal but feels slightly firmer than expected. The implant is palpable but not visible through the skin. |
| III | The breast feels firm and appears visibly distorted. The implant shape may be visible, and the breast can look abnormally round or high. |
| IV | The breast is hard, painful, and visibly distorted. The implant may feel immobile within the capsule. |
Grades I and II generally do not require intervention. Grades III and IV typically warrant surgical treatment, as the condition rarely resolves on its own once it has progressed to these stages.
Risk Factors and Prevention
Several factors influence the likelihood of developing capsular contracture. Implant placement plays a role, as submuscular positioning has been associated with lower contracture rates compared to subglandular placement in multiple studies. How long implants have been in place also matters, as the cumulative risk increases over time.
Surgical technique is important. Using a "no-touch" technique, irrigating the implant pocket with antibiotic solution, and careful haemostasis during surgery all help reduce the risk of biofilm formation and haematoma, two of the most strongly implicated triggers.
Implant surface texture has also been studied as a factor. Textured implants were initially developed partly to reduce contracture rates, and some evidence supports a lower incidence with textured surfaces. However, this must be weighed against other clinical considerations your surgeon will discuss with you.
Post-operative factors such as implant displacement exercises (where recommended by your surgeon) and wearing the appropriate support garment during healing may also contribute to maintaining a soft capsule.
Treatment Options
For mild contracture (Baker II), many surgeons recommend monitoring and, in some cases, non-surgical approaches such as massage techniques or medication. Evidence for non-surgical treatments is mixed, and results vary.
For grades III and IV, surgery is the standard approach. The most common procedures are capsulotomy, where the capsule is scored or partially released to loosen the constriction, and capsulectomy, where the entire capsule is surgically removed. Capsulectomy is generally considered the more definitive option, particularly for grade IV cases.
During revision surgery, the surgeon may change the implant pocket from subglandular to submuscular if the original placement contributed to the problem. The implant itself is typically replaced at the same time. In some cases, patients choose explant (implant removal without replacement).
If you notice increasing firmness, shape changes, or discomfort in either breast, consult your surgeon for an assessment. Early evaluation gives you more options and allows for planned, elective revision.



